With lockdown easing up and botanical gardens and parks open for hiking, people are active and getting some fresh air in the outdoors. With around 175 different snake species in southern Africa, there is a real chance that while hiking, one may encounter a snake. While very few fatal snakebites are recorded in South Africa – around 12 per year – it is important to reduce the risk of a snakebite and to know what to do if someone is bitten.
Nine out of ten serious snakebites in Southern Africa result in cytotoxic symptoms – pain, gradual swelling, blistering and, in some instances, tissue damage. Most of our fatal bites are from Black Mamba and Cape Cobra envenomation – the venom of these snakes is predominantly neurotoxic, causing progressive weakness that ultimately compromises breathing.
When hiking, stay on footpaths, watch where you are walking, step onto rocks and logs and be careful where you put your hands, either when stopping for a rest or when gripping onto rocks to climb up or down inclines. The majority of snakebites are well below the knee and wearing proper snake gaiters will provide good protection against most snakebites. Modern snake gaiters are light (around 400 grams a pair), flexible and comfortable, even on long hikes.
Be prepared for emergencies when planning a hike, make sure you have the necessary emergency numbers on your cell phone and remember that the international emergency number - 112 - works even if you do not have airtime or signal. Check out the Hiker' First Aid Kits on the website www.africansnakebiteinstitute.com and download the free ASI App, ASI Snakes (http://bit.ly/snakebiteapp).
As most snakebites are from snakes with cytotoxic venom, there is little one can do other than safely getting the victim to the nearest medical facility. Meeting a private ambulance halfway often makes sense as paramedics are far better equipped to assist victims.
ASI Snake Gaiters- Lite
Tried and Tested -the ASI Lightweight Snake Gaiters have been tested against bites from the Puff Adder, Cape Cobra, Snouted Cobra and Black Mamba with no penetration during testing. Ideal for hikers, birders, fly-fishermen, geologists, bush-clearing teams, hunters and mountain biking.
Price R1850.00
Never use an arterial tourniquet. Dr. David Warrell, the World Health Organisation’s snakebite expert and an Oxford university professor, has the following to say about arterial tourniquets:
“Arterial (tight) tourniquets applied at pressures above systolic blood pressure are far too dangerous ever to be recommended as I have made clear in all my publications. If applied at sufficient pressure to the upper arm or thigh where there is no interosseous blood supply, they can cause total ischaemia distally with a high risk of gangrene after as little as 30 minutes.”
First Aid for Snakebite
For cytotoxic envenomation, which will include bites from snakes such as the Puff Adder, Rhombic Night Adder, Bibron’s Stiletto Snake and the Mozambique Spitting Cobra, there is virtually nothing that a first aider can do other than getting the victim to the nearest hospital. DO NOT cut and try to suck out venom or put any pressure bandages or tourniquet on. Get the victim to hospital. If you are hours away from the nearest help, either send someone to call for help or walk back to the vehicles (do not run). Cytotoxic venoms are slow-acting and getting to a hospital within an hour or two will greatly benefit the victim. In serious bites, the longer it takes for the victim to be treated with antivenom (if required), the more severe the tissue damage. Bites from these snakes are seldom fatal.
For predominantly neurotoxic bites (Black Mamba or Cape Cobra) it is vital to get the victim to a hospital urgently and before breathing is compromised. Victims soon experience pins and needles in the lips, have difficulty swallowing, sweat profusely, get nauseous and may vomit, experience ptosis and dilated pupils and eventually breathing becomes more and more laboured.
The following first aid measures may be considered:
Pressure Pads
In a confirmed Black Mamba or Cape Cobra bite, one can immediately put a pressure pad directly on the bite. Such a pad, made of rubber, cloth or cotton wool and measuring roughly 6 x 3 x 3 cm, should be bandaged as tight as one would for a sprained ankle and with a non-elastic bandage. It can be applied anywhere on the body. Such a pressure pad may trap the venom in the bitten area and delay the rate at which it spreads and does damage. Experiments on pressure pads have been done for more than 40 years and with good results, but this form of first aid has had little appeal and for no good reason.
Pressure Immobilisation
The use of pressure bandages has been around since the 1980s but is difficult to use effectively without training. If pressure bandages are going to be added to a first aid kit, ensure that they are designed for first aid in snakebite and have printed rectangles along the length of the bandages.
If you are more than an hour or two from the closest medical facility after a suspected Black Mamba or Cape Cobra bite, consider applying a pressure bandage to the affected limb whilst transporting the patient to hospital. Do not apply a pressure bandage if swelling is already present or beginning to form, or if it is known that the victim was bitten by a snake with a predominantly cytotoxic venom that may cause excessive swelling, such as an adder, Mozambique Spitting Cobra or Stiletto Snake. The purpose of the pressure bandage is to apply pressure on the lymphatic system as snake venom is initially absorbed and transported largely through the lymphatic system. If correctly applied, a pressure bandage may slow down the rate at which venom spreads via the lymphatics and buy the victim some time. Like many aspects of first aid in snakebite, there are those that have no faith in pressure immobilisation while others accept it and use it widely. It is standard procedure for medical personnel in South Africa for neurotoxic envenomation. If there is evidence of local swelling (cytotoxicity) a pressure bandage should not be applied.
ASI Snake Scales Face Mask
An easy to wear, adult tapered face mask, with elasticated ear loops.
Price R60.00
Immobilise the affected limb and immediately apply firm pressure to the site of the bite, then wrap the site tightly as you would for a sprained ankle and continue to wrap the entire limb from the bite towards the heart.
For a pressure bandage to work effectively, a specific pressure of around 50 – 70 mm Hg should be applied, and this is no easy task. It is best to use a bandage that has rectangles printed on it – the bandage is stretched until the rectangles become squares and the right pressure is then achieved.
To minimise movement, splint the limb and if the bite is on a leg, wrap another bandage around both legs. Loosen the bandage if there is severe swelling, but do not remove it.
If the bite is on a hand or arm, straighten the arm and once the pressure bandage has been applied, and splint the straightened arm to minimise movement.
Please note that the idea of pressure bandages is not to cut off blood circulation – if you press on a nail there should still be signs of good capillary refill (within 2 seconds).
The pressure bandage should stay in place until such time as the patient reaches a medical facility and should only be removed by medical staff.
Important: Do not waste valuable time applying a pressure bandage – this can be done while the patient is being transported to the nearest medical facility.
Respiratory Support
In serious snakebite cases involving snakes with predominantly neurotoxic venom such as the Black Mamba or Cape Cobra, the patient may soon experience trouble breathing. The onset of breathing difficulty usually takes around one to three hours but in rare cases, it can be in less than 30 minutes. This is a very serious medical condition and respiratory support could be lifesaving.
Mouth-to-mouth resuscitation may be beneficial, but a barrier device may be is required if you do not know the patient.
If a patient stops breathing, it is vital to start with rescue breathing immediately. While most first aid kits have a face mask (a smallish plastic one-way valve situated in the centre of a piece of plastic), they are not easy to use. A far better piece of equipment is a pocket mask.
Pocket Mask
It is easy to get a good seal over the mouth and nose of a patient with a pocket mask and rescue breathing is provided at one breath every six seconds in adults, one breath every five seconds in children and one breath every four seconds in infants. Each breath is given slowly over one second and just enough air for the chest to rise – nothing more.
While providing respiratory support via mouth-to-mouth breathing using a pocket mask is effective, it is also tiring and will be difficult to maintain for very long periods.
Bag Valve Mask Reserve
If possible, the use of a bag valve mask reserve is far more effective and can be used much longer. Having said that, one ideally needs two trained people to effectively use a bag valve mask.
To effectively use a bag valve mask, the patient needs to be laid on his or her back with a rescue breather behind the head. A good seal is required over the mouth and nose with two hands on the face mask, the head tilted back and the chin lifted. Tilting the head back and lifting the chin is important as it pulls the tongue away, off of the throat. The second rescue breather should ideally be on the side of the patient squeezing air into the lungs of the patient every six seconds in adults, five seconds in children and four seconds in infants. The bag is squeezed gently over a period of one second with just enough air to see a chest rise.
Using a bag valve mask in a vehicle while transporting the patient to hospital is no easy task. Another complication, especially in Black Mamba bites, is saliva accumulating in the mouth as the tongue becomes paralysed and no longer functions. In such instances it is best to drain excessive saliva from the mouth using a hand pump or laying the patient on his or her side to allow the saliva to drain.
The advantages of using a bag valve mask:
It reduces the risk of contamination of bodily fluids as you no longer have to place your face close to the patient’s.
It reduces rescuer fatigue and therefore can be used effectively for long periods of time.
Disadvantages of using a bag valve mask:
Bag valve masks can only be used effectively by trained people.
The greatest difficulty is getting a proper seal on the face and this has an effect on the efficiency of the bag valve mask and the amount of oxygen that the patient gets. Men with beards are quite difficult to bag and infants need an infant bag valve mask.
For single operators it is difficult to get a good seal using one hand, tilting the head backwards to open up the airway and getting the chin to lift while the other hand is needed to squeeze air into the lungs.
If available, oxygen can be connected to the mask. Oxygen may be set at 5 – 8 litres per minute for rescue breathing but if full CPR is required, a flow of 15 litres per minute may be more beneficial.
The common spitting snakes in South Africa are the Mozambique Spitting Cobra (M’Fezi) and the Rinkhals. Both snakes spray their venom up to a distance of three meters and do so in self-defence to temporarily blind their attacker so that they can make a quick escape. The other spitting snakes in southern Africa are the Black Spitting Cobra that occurs in the Western Cape and the Northern Cape and into Namibia, the Zebra Cobra that occurs from southern Namibia northwards into Angola and the Black-neck Spitting Cobra that enters Namibia in the north. All of these snakes also bite using the same venom that they spit.
Although spitting snakes accurately aim for the region of the eyes, the venom diffuses into a spray over a wide area and will get onto your hair, face, arms, neck and chest. Venom in the eyes causes immediate pain and must be rinsed with water under a tap as quickly as possible. The first reaction of the victim will be to keep the eyes closed tightly due to the pain, so rinsing the eyes is no easy task. It is best to flush the eyes with copious amounts of water. The production of tears will start immediately and will help somewhat to rinse excess venom. Bear in mind that you are not trying to neutralise venom but to flush away excess venom. The damage to the cornea and eyelids is done virtually instantly and the victim should be transported to a medical facility. Doctors treat the eyes with local anaesthetic, will examine the eyes for corneal damage and may treat the eyes with antibiotic drops or cream (something like Chloramphenicol) to prevent secondary infection of the damaged cornea.
Diluted antivenom should not be used. If water is not available, other bland liquids can be used to flush the eyes.
If the eyes are flushed with water immediately after being spat and the victim taken to a medical facility for treatment, the chances of permanent damage to the eyes are exceptionally remote.
ASI Standard Snake Hook
One of the best selling snake hooks in Africa – the ASI Standard Snake Hook is made from a new steel shaft with a new ASI grip and an aluminium hook that is attached using aeronautical glue. Tested to lift up to 5 kg.
Price R295.00
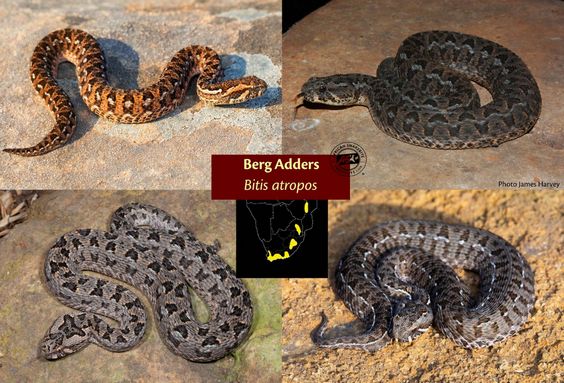
Be careful of Berg Adders – they are small and bite readily. Their venom is quite unique, causing pain and swelling, blurred vision, dilated pupils, loss of smelling and taste and eventually affecting breathing. Most victims need to be ventilated for a few days but only after about 5 – 8 hours after a bite. A Berg Adder bite victim must be taken to hospital urgently – do not apply bandages.
For more detailed information on first aid for snakebite, visit the African Snakebite Institute website www.africansnakebiteinstitute.com
Johan Marais is the author of various books on reptiles including the best-seller A Complete Guide to Snakes of Southern Africa. He is a popular public speaker and offers a variety of courses including Snake Awareness, Scorpion Awareness and Venomous Snake Handling. Johan is accredited by the International Society of Zoological Sciences (ISZS) and is a Field Guides Association of Southern Africa (FGASA) and Travel Doctor-approved service provider. His courses are also accredited by the Health Professions Council of South Africa (HPCSA). Johan is a qualified instructor for the Emergency Care & Safety Institute, in Oxygen Administration and Wilderness First Aid.